Gallbladder pathology is most commonly non-neoplastic,
including common disorders as gallstones,
acute and chronic cholecystitis and cholecystosis (adenomyomatosis and cholesterolosis).
Much more uncommon is the neoplastic pathology,
that can be either malignant,
more frequently gallbladder adenocarcinoma,
or potentially malignant,
as adenomas.
( Fig. 2 )
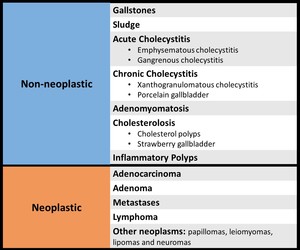
Fig. 2: Gallbladder disorders
The imaging findings were reviewed,
with a sonographic-pathologic correlation,
based on the acknowledgement of basic concepts about the interaction between ultrasound and tissue.
1. Non-neoplastic - Common
• Gallstones - Intraluminal structures that are [3,6]: ( Fig. 3 )
- Echogenic
- Mobile
- Associated with an acoustic shadow ( Fig. 4 )
- Echogenic surface with acoustic shadow in the expected gallbladder location (gallbladder is filled with gallstones)

Fig. 3: Gallstones appear as echogenic, mobile, shadowing structures in the dependent portion of gallbladder (A.). Sometimes, the gallbladder becomes filled with gallstones (C.) and appears as an echogenic surface with acoustic shadow in the gallbladder location(B.)
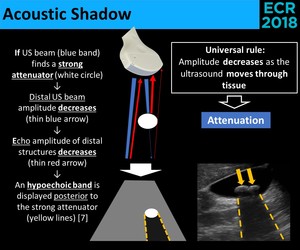
Fig. 4: Physical principles of the acoustic shadow.
⇒ Gallstones < 3-5 mm may not have an acoustic shadow!
• Sludge - Cholesterol crystals and bilirrubinate granules that appear as low to high-level echoes,
without a shadow [3,6]: ( Fig. 5 )
- Bile-sludge level (more frequently)
- Sludge totally fills the gallbladder
- Sludge aggregates
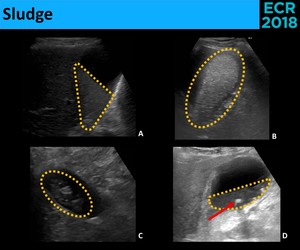
Fig. 5: Biliary sludge can appear as low (A.) to high-level (B.) echoes and assume different forms, including sludge-bile level (A.), a completely filled gallbladder (B.) and tumefactive sludge (C.). Gallstones (red arrow) can be seen within the sludge (D.)
• Acute Cholecystitis - Inflammatory process of the gallbladder that,
without treatment,
can progress to necrosis and perforation [3].
⇒ Treatment of choice – Cholecystectomy in the first 48-72h
⇒ More frequently caused by an impacted stone
⇒ Sonographic criteria [3,6,8]: ( Fig. 6 )
- Gallstones
- Wall thickening (≥3 mm)
- Gallbladder enlargement (transverse diameter > 4 cm)
- Pericholecystic fluid (++ near fundus)
- Impacted stone
- Sonographic Murphy sign
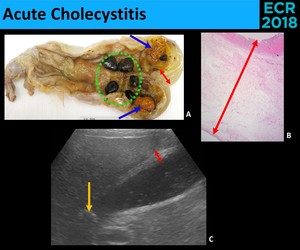
Fig. 6: Acute Cholecystitis. Macroscopic (A.), microscopic (B.) and sonographic (C.) examples of diagnostic criteria of acute cholecystitis: gallstones (green circle), impacted gallstone (yellow arrow), biliary sludge (blue arrows) and thickening of the galllbladder wall (red arrows).
There are no pathognomonic signs! → Combination of the presence of sonographic signs in the appropriate clinical setting increases the diagnostic confidence.
[3,6]
- Gangrenous Cholecystitis - Necrosis of the gallbladder [6]
⇒ implies a more advanced stage of disease
↓
More urgent intervention!
⇒ Sonographic signs [3,6]: ( Fig. 7 )
• Pericholecystic fluid
• Sloughed mucosal membranes
• Wall disruption
• Wall ulceration
• Collections within the wall
• Focal wall bulge
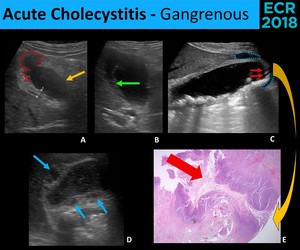
Fig. 7: Gangrenous cholecystitis. Sonographic (A., B., C. and D.) and microscopic (E.) findings of gangrenous cholecystitis: wall ulceration (red dotted line), focal wall bulge (yellow arrow), sloughed mucosal membranes (green arrow), wall disruption (red arrows), pericholecystic fluid (blue dotted line) and collections within the wall (blue arrows).
Murphy Sign is frequently absent! (necrosis of the nerve supply)
- Emphysematous Cholecystitis - Infection with gas-forming organisms → Gas in the wall and lumen of gallbladder [3,6] ( Fig. 8 )
⇒ Uncommon
⇒ ++ Elderly men
⇒ ++ Diabetics
⇒ Often acalculous
⇒ Perforation is much more common [3,6]
↓
Urgent cholecystectomy for all patients!
⇒ Sonographic appearance:
• Echogenic surface in a nondependent location
• Dirty acoustic shadow
• Ring-down artifact (not always demonstrable) → Reliable sign!
• Pneumobilia
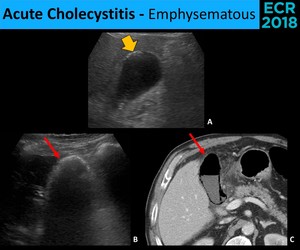
Fig. 8: Emphysematous cholecystitis has different sonographic appearances accordingly to the amount of gas in the wall and lumen of the gallbladder. A little amount of gas is seen as hyperechogenic areas (yellow arrow) in the nondependent portion of the gallbladder, associated with an acoustic shadow that allows the visualization of the gallbladder lumen and posterior wall (A.). Larger amounts of gas will appear as an hyperechogenic arc (red arrow) that totally overshadow the posterior structures (B. e C.).
- Acalculous Cholecystitis - represents a minority of the acute cholecystitis,
being much more frequent in critically ill or injured patients [3,6]
⇒ Limited sonographic evaluation:
• Absence of gallstones
• Gallbladder abnormalities of other causes than cholecystitis
→ Gallbladder distention
→ Wall thickening
→ Sludge
→ Pericholecystic fluid
• Unreliable evaluation of sonographic Murphy's sign
(unresponsive patients and patients taking analgesic medication)
• Chronic Cholecystitis - inflammatory process of the gallbladder,
almost always in the setting of cholelithiasis.
It can lead to fibrosis.
⇒ Complications:
- Acute cholecystitis
- Gallbladder carcinoma
- Biliary-enteric fistula → Gallstone Ileus
⇓
Uncomplicated chronic cholecystitis should be treated with elective cholecystectomy. [8]
⇒ Sonographic criteria [8]: ( Fig. 9 )
- Gallstones
- Wall thickening
- Contracted or distended gallbladder
Without the other signs of acute cholecystitis!
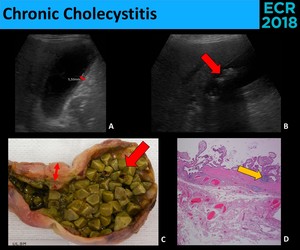
Fig. 9: Chronic Cholecystitis has only inespecific sonografic findings (A. and B.), as wall thickening (red thin arrows) and the presence of gallstones (red thick arrow), in keeping with the macroscopic appearance (C.). The diagnosis usually relies on microscopy (D.), where the detection of lymphoid aggregates (yellow arrow) is one of diagnostic features.
- Porcelain Gallbladder - Calcification of the gallbladder wall.
⇒ Associated with chronic gallbladder inflammation and gallstones
⇒ Questionable association with gallbladder carcinoma
• Association with carcinoma is more evident with scattered calcifications (compared to transmural calcifications)
⇓
Prophylactic cholecystectomy is no longer the standard of care [3] and follow-up isn't recommended [9].
⇒ Sonographic appearance [3,6]: ( Fig. 10 )
• Hyperechoic segments of the gallbladder wall (early phase)
• Hyperechoic arc with posterior acoustic shadow (partial or dense,
accordingly to the calcification level)
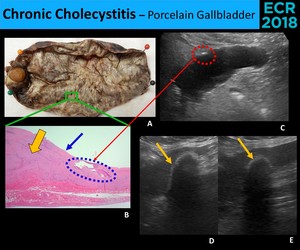
Fig. 10: Sonographic findings of porcelain gallbladder vary with the amount of calcium deposition. In an early stage, there are only focal spots of calcium (blue circle) (A., B. and C.), appearing as echogenic foci or small echogenic areas (red circle) which may not be associated with acoustic shadow (if there isn’t enough calcium). Transmural deposition of calcium in the entire gallbladder wall will create an echogenic arc with a dense posterior acoustic shadow (thin yellow arrow) (D. and E.) (A., B. and C. - Completely hyalinized wall (yellow thick arrow) without mucosal (blue arrow) resulting in a hard and trabeculated gallbladder at macroscopy and in a very irregular contour of the gallbladder at sonography)
- Xanthogranulomatous Cholecystitis - Active and destructive inflammatory process,
characterized by the presence of nodules with lipid-laden macrophages in the gallbladder wall.
[3,6,10]
⇒ It can affect the adjacent structures,
causing complications as:
• Perforation of the gallbladder
• Strictures of the biliary tract
• Hepatic abscesses
• Fistulas (to duodenum,
liver,
stomach,
colon,
skin)
• Ascending cholangitis
• Mirizzi syndrome
⇓
Xanthogranulomatous cholecystitis should be treated with elective open cholecystectomy.
[11]
⇒ Broad spectrum of appearances → Sonographic signs [3,8,
10]:
( Fig. 11 )
• Gallstones
• Thickening of the gallbladder wall (focal or diffuse)
• Hypoechoic nodules (6-12 mm) or bands in the gallbladder wall
• Gallbladder mass
• Subhepatic fluid collection
• Obscure border between gallbladder and liver
• Gas in the biliary tree
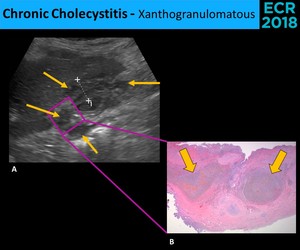
Fig. 11: The sonographic diagnosis of xanthogranulomatous cholecystitis (A.) is frequently impossible, because the most common findings, as the wall thickening (cursors), are nonspecific. The most characteristic finding is the presence of intramural hypoechoic nodules or bands (thin arrows), corresponding to the nodules with lipid-laden macrophages (thick arrows) visualized in the microscopy (B.)
Sonographic findings are similar to other cholecystitis forms and gallbladder carcinoma!
• Adenomyomatosis - Mucosal hyperplasia + thickening of the muscular layer
⇒ Mucosal herniation into the muscle layer → Rokitansky-Aschoff sinuses (RAS)
⇒ RAS frequently contain cholesterol crystals [3]
⇒ Sonographic appearance [3,6]: ( Fig. 12 )
- Wall thickening → Three distinct forms:
• Diffuse wall thickening
• Focal mass (adenomyoma)
• Focal annular thickening
- Comet-tail artifacts (most common and obvious sign) ( Fig. 13 )
- Hypoechoic/cystic spaces on the wall
- Echogenic foci in the wall
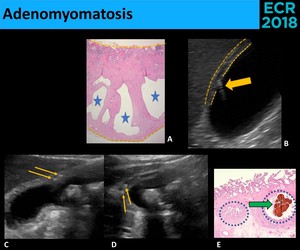
Fig. 12: Adenomyomatosis is characterized by thickening of the muscle layer and mucosal hyperplasia, with mucosal protruding into the muscle layer (A.), forming the Rokitansky-Aschoff sinuses (RAS) (Blue stars). Sonographically (B., C. and D.), a parietal thickening is seen (yellow dotted line – parietal surfaces), often with comet-tail artifacts (yellow thick arrow), caused by cholesterol crystals. Often, the microscopy (E.) shows cholesterol crystals (green thick arrow) inside RAS (blue circle), in keeping with the echogenic foci (thin yellow arrows) seen inside little cystic spaces at sonography.
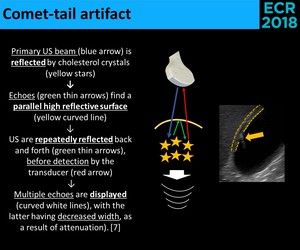
Fig. 13: Physical principles of the comet-tail artifact.
• Cholesterolosis - Deposition of triglycerides and cholesterol in the lamina propria of the gallbladder [3]
⇒ Two forms:
1 - Planar deposition (more frequently) – “Strawberry gallbladder”
2 - Polypoid – Cholesterol polyps (the most common type of polyps)
- Strawberry Gallbladder - Without sonographic changes ( Fig. 14 )

Fig. 14: Strawberry gallbladder owes its name to the stippled appearance of the mucosal (A.). Sonographically, there are any changes (B.).
- Cholesterol Polyps - Enlarged papillary fronds with lipid-laden macrophages,
attached to the wall by a stalk → They’re not true neoplasms! [1]
⇒ Sonographic appearance [3,4,6]: ( Fig. 15 )
• Intraluminal ovoid lesions,
attached to the gallbladder wall
• ++ ≤ 5 mm; rarely > 10 mm
• Usually multiples,
but frequently only the largest is seen
• Ball-on-the-wall sign
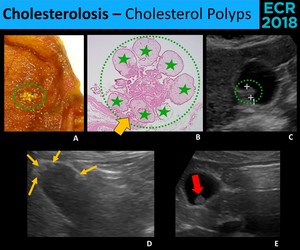
Fig. 15: Cholesterol polyps (green dotted circles) are the most common type of gallbladder polyps. They are constituted of papillary fronds plentous of lipid-laden macrophages (green stars), therefore they aren’t true neoplasms. (A. and B.) Sonographically (C., D. and E.), cholesterol polyps appear as echogenic, round and usually multiple (thin arrows) images. Although cholesterol polyps usually have a stalk (thick yellow arrow), often it is too thin to be seen, and the polyp looks like a “ball-on-the-wall” (red arrow).
2. Neoplastic –Uncommon
• Adenoma - Benign neoplasms,
with a premalignant potential [6]
⇒ Sonographic appearance [6]: ( Fig. 16 )
- Polypoid pedunculated lesions
- ++ solitary and larger than cholesterol polyps
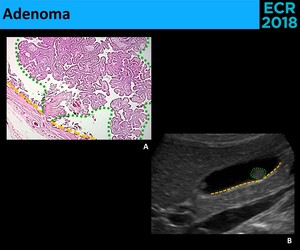
Fig. 16: 16 – Adenomas are an infrequent type of gallbladder polyps with a premalignant potential. They consist of epithelial proliferation with dysplasia (A.). At ultrasound (B.), they appear usually as polypoid lesions (green circle), similar to cholesterol polyps
• Adenocarcinoma - Poor prognosis if advanced stage (5 year survival: < 25%) [4]
⇒ Gallstones > 3 cm → ↑ 10 fold risk of gallbladder carcinoma [1]
⇒ Sonographic appearance [3,6]: ( Fig. 17 )
- Soft-tissue mass occupying the gallbladder lumen (more commonly)
- Wall thickening (focal or diffuse) → ++ irregular and asymmetric
- Polypoid mass (>> 10 mm) → ++ sessile
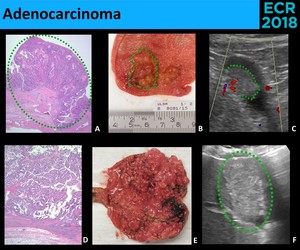
Fig. 17: Like other adenocarcinomas, the pathological diagnosis of gallbladder adenocarcinoma is based on invasion of the Wall (A.) Macroscopically, gallbladder adenocarcinomas (inside greenline/circle) may present as an intraluminal polypoid mass (B. and C.), a totally filled gallbladder with echogenic material (D., E. and F.) or a thickening of the gallbladder wall.
• Metastases - rare cause of polypoid masses [3,6]
⇒ ++ Melanoma
↓
Polyps in patients with melanoma are always suspicious
⇒ Other adenocarcinomas (rarely) ( Fig. 18 )
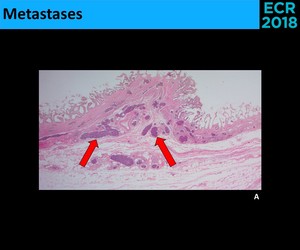
Fig. 18: Microscopic evidence (A.) of gastric adenocarcinoma metastases, with lymphatic permeation (red arrows) in the gallbladder wall.(Cholecystectomy performed in the setting of a gastrectomy; no imagiologic findings were seen in the gallbladder wall prior to the surgery)
⇒ Sonographic appearance [6]:
- Hyperechoic sessile polypoid lesions
- Potentially multiple
- ++ >10 mm
• Lymphoma - Primary lymphomas of the gallbladder are extremely rare.
⇒ More commonly: secondary involvement from adjacent lymph nodes [12]
⇒ Sonographic appearance [13]: ( Fig. 19 )
- Soft-tissue mass occupying the gallbladder lumen
- Polypoid mass
- Wall thickening
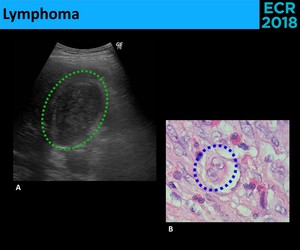
Fig. 19: Ultrasound (A.) shows a soft-tissue mass completely occupying the gallbladder lumen (green circle). The microscopy (B.) allowed the identification of Reed-Stenberg cells (blue circle), diagnosing Hodgkin Lymphoma.
• Other neoplasms: papillomas,
leiomyomas,
lipomas and neuromas
Differential Considerations
• Important concepts (Fig. 20,
Fig. 21, Fig. 22)
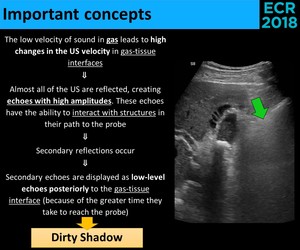
Fig. 20: Physical explanation of the "dirty shadow".
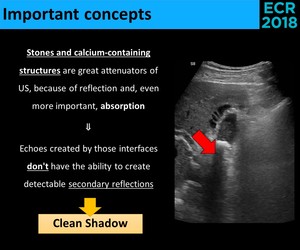
Fig. 21: Physical explanation of the "clean shadow".
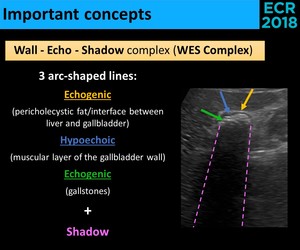
Fig. 22: WES Complex definition.
• Differential diagnosis
- Hyperechoic semilunar image in the gallbladder location (Fig. 23)
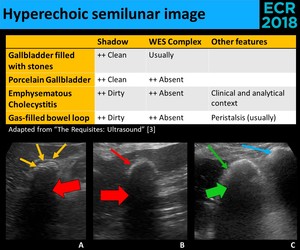
Fig. 23: An hyperechoic semilunar image associated with a shadow in the location of the gallbladder has four major differential diagnosis: a gallbladder completely filled with gallstones (yellow thin arrows) (A.), a porcelain gallbladder (red thin arrow) (B.), an emphysematous cholecystitis (green thin arrow) (C.) and a gas-filled bowel loop (blue arrow), that in cholecystectomized patients may appear in the gallbladder location. A gallbladder filled with stones often shows the WES Complex (yellow thin arrows), distinguishing it from the others. The shadow of the gas (green thick arrow) differs from the shadow of calcium or stones (red thick arrow), because while gas has a dirty shadow, the latter have a clean shadow.
⇒ CT allows the distinction between them.
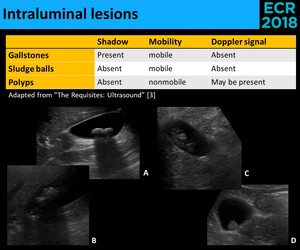
Fig. 24: Intraluminal lesions may correspond to stones (A. and B.) that are mobile and have an acoustic shadow, sludge balls (C.) that are also mobile, but don’t have shadow, or polyps, that are neither mobile or shadowing (D.)
—————————————————————————————————————
Acoustic shadow doesn't always appear → Adjusting the parameters of the ultrasound equipment may transform a non-shadowing stone in a shadowing stone:
• Using higher frequencies (US absorption increases with increasing frequency)
• Using a single focal zone at a proper place (a great number of US interact with the stone,
being attenuated)
——————————————————————————————————————
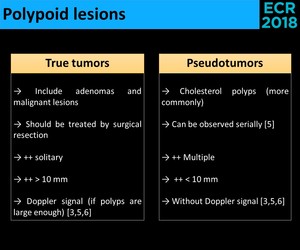
Fig. 25: Polypoid lesions - differential criteria.
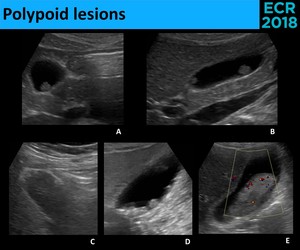
Fig. 26: Polypoid lesions can be either pseudotumors, most commonly cholesterol polyps (A. and C.) or true neoplasms, including lesions with malignant potential, like adenomas (B.), and malignant lesions, with adenocarcinoma being the most common type (D. and E.). Cholesterol polyps appear frequently as a “ball-on-the-wall” lesion, with diameter < 10 mm (A.) and are usually multiple (C.), although these findings can be seen also in true neoplasms (B. and D.). Characteristically, true neoplasms are larger, sessile and solitary lesions and, if larger enough, they can have Doppler signal (E.).
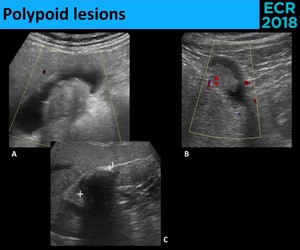
Fig. 27: Doppler signal has its main utility in distinguishing between nonmobile tumefactive sludge (A.) and true neoplasms (B.); the presence of Doppler signal excludes sludge. When the doubt persists, sonographic evaluation in few weeks may demonstrate a change in appearance (C.), confirming the sludge hypothesis.
- Intraluminal echogenic content (Fig. 28)
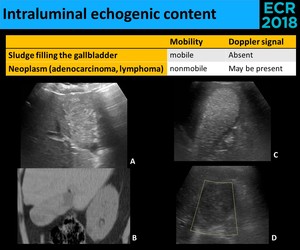
Fig. 28: A gallbladder totally filled with echogenic content presents a diagnostic challenge because the sonographic distinction is often impossible. Distinguishing between a neoplastic lesion (A., B. and D.) and sludge (C.) frequently implies a CT examination. The utility of Doppler signal relies in its positivity, thus the absence of internal vascularity doesn’t exclude a neoplasm (D.), as we can see in the last picture (Hodgkin Lymphoma).
——————————————————————————————————————
⇒ Impossible to distinguish sludge from neoplasms → Follow up examination in several weeks:
• If there is mobility or a change in the appearance ⇒ Sludge
——————————————————————————————————————
⇒ Nonspecific - many conditions can cause increased wall thickness [3,6] ( Fig. 29 ,
Fig. 30 )
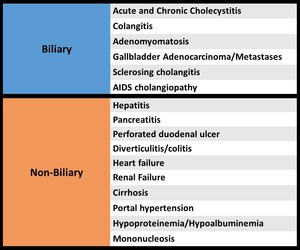
Fig. 29: Causes of wall thickening.
⇒ Major concern: distinguishing between acute cholecystitis (needs emergent treatment) and other processes.
⇓
Distinctive criteria:
- Clinical setting
- Presence/absence of gallstones
- Sonographic Murphy sign
- Signs more specific of a non-biliary etiology:
→ Marked thickening + stratification (++ edematous states)
→ Absence of gallstones + distended gallbladder
- Signs more specific of acute cholecystitis:
→ Multiple noncontiguous hypoechoic collections of fluid in the wall
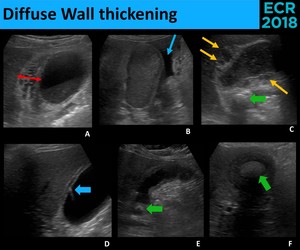
Fig. 30: Diffuse wall thickening has an extensive differential diagnosis, however, the clinical setting and the associated sonographic signs are often sugestive of the underlying etiology. Marked thickening (red arrow) is more common in edematous states, as nephrotic syndrome (A.); ascitis (blue thin arrow) and an heterogeneous hepatic parenchyma are sugestive of cirrhosis (B.); Intramural hypoechoic collections (yellow arrows) with gallstones (green arrow) suggest acute cholecystitis (C.); comet-tail artifact (blue thick arrow) is very specific of adenomyomatosis (D.); the presence of gallstones (green arrow) without RUQ pain and other inflammatory findings may suggest a chronic process (E. – Chronic cholecystitis; F. - Xanthogranulomatous cholecystitis)
• Focal wall thickening ( Fig. 31 )
- Gallbladder Carcinoma - more probable if:
→ Metastatic disease (lymph nodes or peritoneal cavity)
→ Adjacent organs invasion (liver,
bile ducts,
vessels)
→ Presence of Doppler signal
- Metastases - similar to adenocarcinoma
→ Mobile
→ Absence of Doppler signal
→ Non-mobile
→ Cystic spaces
→ Echogenic foci
→ Comet-tail artifact
→ Absence of Doppler signal
- Inflammatory wall thickening
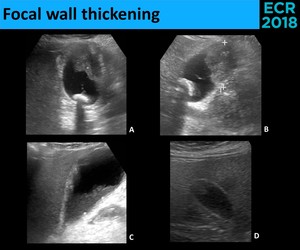
Fig. 31: As with polypoid lesions, the major concern with focal wall thickening is a malignant process. Mobility shoud also be evaluated, with nonmobile lesions being suspicious for neoplasm (A. and B. – Adenocarcinoma) and mobile material being highly sugestive of sludge (C.). It should be kept in mind that pseudotumors (D.) may also appear as a nonmobile focal thickening of the gallbladder wall. (D. - inflammatory polyp)
Note: If focal mass or thickening of the wall without cystic spaces,
echogenic foci or comet-tail artifact or with internal vascularity
⇓
Further investigation! [3]


. Sometimes, the gallbladder becomes filled with gallstones (C.) and appears as an echogenic surface with acoustic shadow in the gallbladder location(B.)")

 to high-level (B.) echoes and assume different forms, including sludge-bile level (A.), a completely filled gallbladder (B.) and tumefactive sludge (C.). Gallstones (red arrow) can be seen within the sludge (D.)")
, microscopic (B.) and sonographic (C.) examples of diagnostic criteria of acute cholecystitis: gallstones (green circle), impacted gallstone (yellow arrow), biliary sludge (blue arrows) and thickening of the galllbladder wall (red arrows).")
 and microscopic (E.) findings of gangrenous cholecystitis: wall ulceration (red dotted line), focal wall bulge (yellow arrow), sloughed mucosal membranes (green arrow), wall disruption (red arrows), pericholecystic fluid (blue dotted line) and collections within the wall (blue arrows).")
 in the nondependent portion of the gallbladder, associated with an acoustic shadow that allows the visualization of the gallbladder lumen and posterior wall (A.). Larger amounts of gas will appear as an hyperechogenic arc (red arrow) that totally overshadow the posterior structures (B. e C.).")
, as wall thickening (red thin arrows) and the presence of gallstones (red thick arrow), in keeping with the macroscopic appearance (C.). The diagnosis usually relies on microscopy (D.), where the detection of lymphoid aggregates (yellow arrow) is one of diagnostic features.")
 (A., B. and C.), appearing as echogenic foci or small echogenic areas (red circle) which may not be associated with acoustic shadow (if there isn’t enough calcium). Transmural deposition of calcium in the entire gallbladder wall will create an echogenic arc with a dense posterior acoustic shadow (thin yellow arrow) (D. and E.) (A., B. and C. - Completely hyalinized wall (yellow thick arrow) without mucosal (blue arrow) resulting in a hard and trabeculated gallbladder at macroscopy and in a very irregular contour of the gallbladder at sonography)")
 is frequently impossible, because the most common findings, as the wall thickening (cursors), are nonspecific. The most characteristic finding is the presence of intramural hypoechoic nodules or bands (thin arrows), corresponding to the nodules with lipid-laden macrophages (thick arrows) visualized in the microscopy (B.)")
, forming the Rokitansky-Aschoff sinuses (RAS) (Blue stars). Sonographically (B., C. and D.), a parietal thickening is seen (yellow dotted line – parietal surfaces), often with comet-tail artifacts (yellow thick arrow), caused by cholesterol crystals. Often, the microscopy (E.) shows cholesterol crystals (green thick arrow) inside RAS (blue circle), in keeping with the echogenic foci (thin yellow arrows) seen inside little cystic spaces at sonography.")

. Sonographically, there are any changes (B.).")
 are the most common type of gallbladder polyps. They are constituted of papillary fronds plentous of lipid-laden macrophages (green stars), therefore they aren’t true neoplasms. (A. and B.) Sonographically (C., D. and E.), cholesterol polyps appear as echogenic, round and usually multiple (thin arrows) images. Although cholesterol polyps usually have a stalk (thick yellow arrow), often it is too thin to be seen, and the polyp looks like a “ball-on-the-wall” (red arrow).")
. At ultrasound (B.), they appear usually as polypoid lesions (green circle), similar to cholesterol polyps")
 Macroscopically, gallbladder adenocarcinomas (inside greenline/circle) may present as an intraluminal polypoid mass (B. and C.), a totally filled gallbladder with echogenic material (D., E. and F.) or a thickening of the gallbladder wall.")
 of gastric adenocarcinoma metastases, with lymphatic permeation (red arrows) in the gallbladder wall.(Cholecystectomy performed in the setting of a gastrectomy; no imagiologic findings were seen in the gallbladder wall prior to the surgery)")
 shows a soft-tissue mass completely occupying the gallbladder lumen (green circle). The microscopy (B.) allowed the identification of Reed-Stenberg cells (blue circle), diagnosing Hodgkin Lymphoma.")



 (A.), a porcelain gallbladder (red thin arrow) (B.), an emphysematous cholecystitis (green thin arrow) (C.) and a gas-filled bowel loop (blue arrow), that in cholecystectomized patients may appear in the gallbladder location. A gallbladder filled with stones often shows the WES Complex (yellow thin arrows), distinguishing it from the others. The shadow of the gas (green thick arrow) differs from the shadow of calcium or stones (red thick arrow), because while gas has a dirty shadow, the latter have a clean shadow.")
 that are mobile and have an acoustic shadow, sludge balls (C.) that are also mobile, but don’t have shadow, or polyps, that are neither mobile or shadowing (D.)")

 or true neoplasms, including lesions with malignant potential, like adenomas (B.), and malignant lesions, with adenocarcinoma being the most common type (D. and E.). Cholesterol polyps appear frequently as a “ball-on-the-wall” lesion, with diameter < 10 mm (A.) and are usually multiple (C.), although these findings can be seen also in true neoplasms (B. and D.). Characteristically, true neoplasms are larger, sessile and solitary lesions and, if larger enough, they can have Doppler signal (E.).")
 and true neoplasms (B.); the presence of Doppler signal excludes sludge. When the doubt persists, sonographic evaluation in few weeks may demonstrate a change in appearance (C.), confirming the sludge hypothesis.")
 and sludge (C.) frequently implies a CT examination. The utility of Doppler signal relies in its positivity, thus the absence of internal vascularity doesn’t exclude a neoplasm (D.), as we can see in the last picture (Hodgkin Lymphoma).")

 is more common in edematous states, as nephrotic syndrome (A.); ascitis (blue thin arrow) and an heterogeneous hepatic parenchyma are sugestive of cirrhosis (B.); Intramural hypoechoic collections (yellow arrows) with gallstones (green arrow) suggest acute cholecystitis (C.); comet-tail artifact (blue thick arrow) is very specific of adenomyomatosis (D.); the presence of gallstones (green arrow) without RUQ pain and other inflammatory findings may suggest a chronic process (E. – Chronic cholecystitis; F. - Xanthogranulomatous cholecystitis)")
 and mobile material being highly sugestive of sludge (C.). It should be kept in mind that pseudotumors (D.) may also appear as a nonmobile focal thickening of the gallbladder wall. (D. - inflammatory polyp)")